Every time the Democratic Republic of Congo sneezes, East Africa panics, buys thousands of pairs of latex gloves, and sets up temperature guns at border checkpoints.
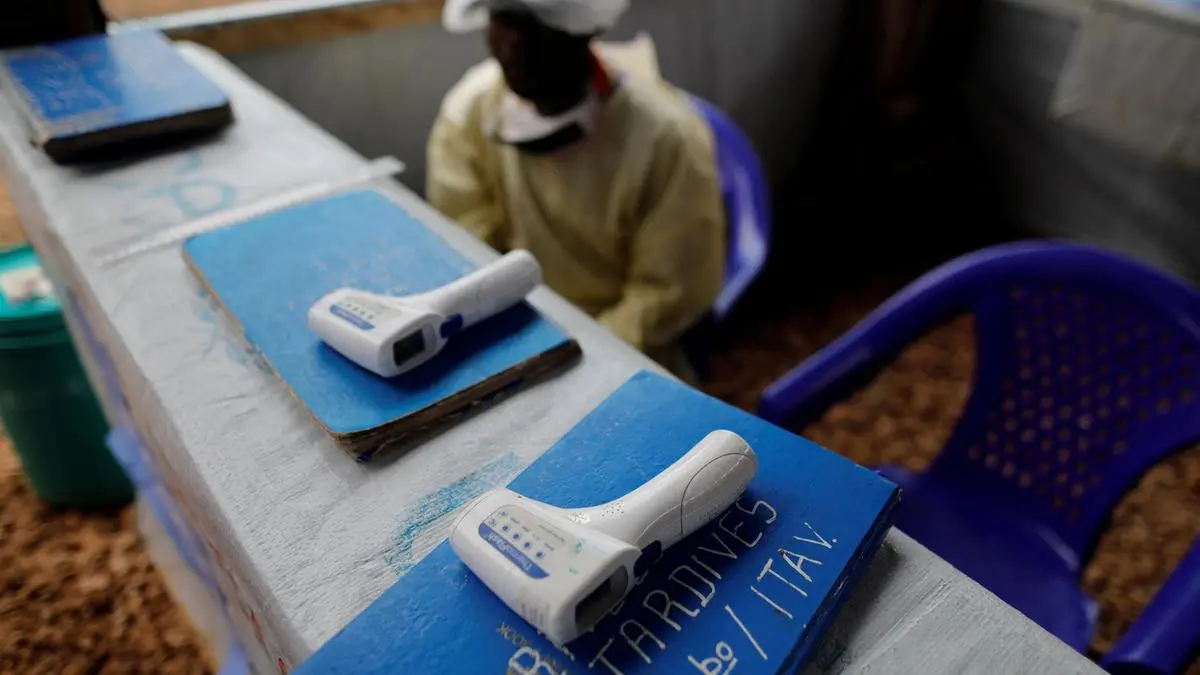
We are seeing it again. Regional headlines scream about Tanzania "intensifying preparedness" and mobilizing health workers along the western border. The public is treated to images of thermal scanners, hastily erected isolation tents, and officials looking serious in high-visibility vests. It looks disciplined. It looks proactive. Meanwhile, you can read other developments here: Epidemiological Bottlenecks and Containment Friction Analysis of the Democratic Republic of Congo Ebola Outbreak.
It is entirely useless.
For two decades, international health agencies and regional ministries have repeated the same playbook. They treat a highly complex, socio-ecological border reality as if it were a modern airport terminal. The standard public health narrative insists that if you deploy enough thermometers, print enough brochures, and station enough guards at official crossings, you can create a biological firebreak. To see the complete picture, check out the detailed analysis by National Institutes of Health.
This is bureaucratic theater. It satisfies donors and calms urban populations, but it ignores how viruses actually move across African borders. The current panic-and-spend cycle does not prevent outbreaks; it merely burns through limited resources that should be funding baseline medical infrastructure.
If we want to actually protect East Africa from Ebola, we have to stop treating the border as a wall and start understanding it as an ecosystem.
The Myth of the Hard Border
Public health strategies are designed by people who live in capital cities and fly into international airports. They view borders as neat lines on a map where travelers present passports and submit to inspections.
The reality on the ground between Tanzania, Burundi, Rwanda, and the DRC is fundamentally different.
The western border of Tanzania spans hundreds of kilometers of dense terrain, rivers, and Lake Tanganyika. This is not a barrier; it is a porous transit zone. Millions of people cross these frontiers every week via unofficial channels, known locally as panya routes (rat paths). They cross to trade fish, visit family, sell charcoal, or seek seasonal agricultural work.
An informal trader carrying a basket of cassava across an unmarked dirt path three miles south of an official checkpoint is not going to stop for a thermal scan. Even at official entry points like Kabanga or Manyovu, a temperature check only catches individuals who are already symptomatic. It does completely nothing to identify someone in the 2-to-21-day incubation period of the virus.
I have spent years tracking how health resources are allocated during these "regional alerts." I have watched millions of dollars in international aid flow into temporary border screening infrastructure, only for those tents to rot and those thermal guns to lose their batteries six months after the media attention shifts.
By centering the containment strategy on border checks, governments create a false sense of security while failing to address the structural vulnerabilities just a few miles inland.
The Flawed Premise of People Also Ask
When regional panic peaks, the internet fills with predictable questions. A look at what people are searching reveals how deeply misunderstood this disease remains.
Can Tanzania stop Ebola at the border?
No. No country can stop a filovirus at a porous land border. The concept of "stopping" Ebola at a frontier assumes the virus respects cartography. When the World Health Organization coordinates responses, the focus often lands heavily on border states because it is a tangible, visible metric. You can count how many people passed through a checkpoint. You cannot easily count the thousands who walked through the bush.
Is East Africa safe from the DRC outbreak?
Safety is the wrong metric. East Africa is always at risk of imported cases, not because of a failure of border guards, but because the economic lifeblood of the region relies on cross-border movement. The moment you attempt to shut down these movements completely, you destroy the local economy, drive the trade deeper into the shadows, and guarantee that an infected person will hide from authorities rather than seek care.
How does Ebola spread to neighboring countries?
It spreads through trucks, boats, and footpaths. It moves with the truck driver hauling goods from Goma to the port of Dar es Salaam. It moves with the fisherman crossing Lake Tanganyika at midnight. It does not wait in line at immigration.
The High Cost of the Panic Cycle
When a country declares an Ebola alert, the funding mechanism shifts into emergency mode. Money is reallocated from routine health services to fund rapid response teams, isolation centers, and border sensitization campaigns.
This looks like decisive leadership. In reality, it is a catastrophic misallocation of capital.
Consider what happens to local health systems during these periods. Resources are stripped from maternal health clinics, malaria prevention programs, and routine childhood immunization drives to fund a hypothetical threat. In a region where malaria, tuberculosis, and acute watery diarrhea kill tens of thousands of people annually, diverting funds to build empty Ebola isolation wards along a border is a net negative for public health.
Worse, it erodes trust.
When teams of health workers arrive in rural villages wearing full personal protective equipment (PPE) to talk about a disease that no one in that village has ever seen, it creates panic. If those same villages lack basic clean water, functional roads, or antibiotics for routine infections, the community views the sudden influx of Ebola funding with suspicion. They see an elite obsession with a terrifying disease, while their daily, mundane causes of death are ignored.
True resilience does not come from specialized Ebola units that sit empty 99% of the time. It comes from having a functional, well-stocked clinic every twenty kilometers that can detect any unusual cluster of symptoms, whether it is Ebola, Marburg, or a novel strain of influenza.
Decentralization and the Power of the Local Clinic
If border screening is a failure, what actually works? The answer lies in shifting the focus from peripheral lines to internal nodes.
The definitive textbook on outbreak management was not written in a Geneva boardroom; it was written in the mud of West Africa during the 2014–2016 epidemic and refined in the dense forests of North Kivu. The lesson from those interventions is clear: outbreaks are contained by local communities, not by national borders.
Instead of spending capital on border checkpoints, resources must be permanently decentralized to primary healthcare facilities within the high-risk zones.
| Intervention Strategy | Traditional Border Focus (Flawed) | Community Node Focus (Superior) |
|---|---|---|
| Primary Tool | Thermal scanners at major crossings | Well-paid, permanent community health workers |
| Data Source | Immigration logs | Local pharmacy sales and traditional healer networks |
| Resource Status | Temporary, donor-funded emergency spikes | Permanent integration into rural clinic budgets |
| Community Trust | Low (seen as state surveillance) | High (integrated into daily healthcare delivery) |
When you train a local nurse or a community health worker to recognize the early signs of hemorrhagic fever, you create a permanent sensor. If an infected trader bypasses the border checkpoint via a panya route and falls ill three days later in a Tanzanian village, they will not go back to the border. They will go to the local dispensary or a traditional healer.
If that local dispenser is untrained, underpaid, and lacks basic gloves, they will treat the patient for malaria, become infected themselves, and amplify the outbreak. If that dispenser is trained and equipped as part of a permanent health system upgrade, they will isolate the patient immediately.
Containment happens at the first point of care, not at the political boundary.
The Traditional Healer Blindspot
There is a glaring omission in standard ministry guidelines: the role of informal healthcare providers.
In rural East Africa, a significant percentage of the population consults traditional healers or faith healers before ever stepping foot in a government dispensary. When a patient presents with sudden, severe illness, vomiting, or bleeding, they are frequently taken to a healer who operates outside the formal surveillance network.
During the 2018–2020 outbreak in the eastern DRC, traditional healers became major vectors of transmission because they were completely excluded from the initial training and distribution of protective gear.
Any preparedness strategy that does not actively integrate traditional healers, local pharmacists, and drug shop operators into the surveillance network is mathematically guaranteed to fail. They are the actual frontline. The customs officer at the border post is just an onlooker.
Stop Preparing, Start Building
The phrase "intensifying preparedness" is a bureaucratic euphemism for doing the same ineffective things with more urgency. It allows ministries to issue press releases and satisfy international health regulations without fixing the underlying vulnerabilities of their health systems.
We must accept the downside of a truly effective approach: it is slow, it is expensive, and it does not make for dramatic television coverage. It requires paying rural health workers a living wage so they do not abandon their posts. It requires ensuring that every remote clinic has a reliable supply of clean water, electricity, and basic personal protective equipment every day of the year, not just during an international crisis.
It means stopping the specialized Ebola drills and instead fixing the supply chains that leave rural dispensaries without stock of basic antibiotics for months at a time.
If a system cannot reliably deliver paracetamol and clean needles to a village clinic in Kagera or Kigoma on a quiet Tuesday in May, it will not stop an Ebola outbreak when the crisis hits.
The theatrical deployments at the border checkpoints need to be dismantled. The scanners should be packed away. The funding must be stripped from the borders and pushed down to the rural clinics, the community health networks, and the informal healers who actually hold the line.
Until we stop funding the illusion of containment and start financing the reality of basic medicine, East Africa will remain permanently vulnerable to the next virus that walks across the bush.